Clinical Manifestations
CD is the most common form of focal dystonia. Few epidemiological studies exist that estimate the incidence and prevalence of CD; separate studies of different geographical locations and times show the prevalence to be between nine and 30 per 100,000 individuals in the US.1,4 Currently, the prevalence of cervical dystonia in the US is estimated to be greater than 90,000. Other studies show that its prevalence differs among ethnic groups.5-7 Claypool et al. in 1995 reported an incidence of 1.2 per 100,000, while an incidence of 5.4 per 100,000 was published in a practice-based survey of dystonia in Munich.7 Women are affected 1.3- to 2-fold more often than men. CD can occur at any time of life, but most individuals experience their first symptoms in middle age. Chen et al. reviewed the clinical details of CD in 266 patients. In their study, the median age of onset was 41 years, with a female-to-male ratio of 1.9 to 1. They found a familial history of dystonia in 12% of cases. Remission was achieved in 9.8% of patients.8
Pathophysiology
The pathophysiology of idiopathic CD is not well understood. Recent studies have explained the pathogenesis of CD at the peripheral and central nervous system (CNS) level. Although any muscle in the neck may be involved, the common muscles associated with abnormal head posture are well described.9,10 CD, like other focal dystonias, is a syndrome of abnormality in central motor processing. Head tremor and neck spasms are cardinal clinical features in patients with CD.8,11 The majority of affected patients complain of pain, which is not common in other types of focal dystonia other than writer’s cramp. Hand and arm tremor may be seen in patients with torticollis.11-13 In certain cases, head, arm, or trunk tremor can be the initial presenting symptom and sometimes the isolated manifestation of torticollis.14
Clinical Manifestation
Most patients with torticollis find a sensory trick a useful tool to control or eliminate their symptoms. A sensory trick has been called a ‘geste antagoniste’ and is a unique feature of dystonia. Typically, placing the hand on the chin, the side of the face, or the back of the neck reduces muscle contraction in CD without applying mechanical pressure. In some patients, thinking about a geste antagoniste eliminates or diminishes symptoms just the same as actually performing the sensory trick.15 Although the use of a geste antagoniste is reported in more than 50% of patients with CD,11 its mechanism of action is still unknown.
Management
Medical Therapy
The efficacy of oral drug therapy is limited and many different medication trials show a low rate of success in controlling the symptoms of CD.16
Botulinum Toxin
Seven serotypes of botulinum toxin have been identified. Their specific action is at cholinergic synapses to block pre-synaptic release of acetylcholine. By inhibiting the release of acetylcholine at the neuromuscular junction, they decrease inappropriate co-contraction of agonist and antagonist muscles in dystonia. Over the last 15 years, intramuscular injection of botulinum toxin has become the treatment of choice for patients with CD. Injection of the toxin into appropriate neck muscles relieves torticollis symptoms. Various controlled trials show 60–90% improvement following intramuscular toxin injection.17-23 Patients usually notice improvement of their symptoms starting five to 10 days after injection, with lasting benefit for three to four months. Peak benefit typically occurs within two to four weeks of injection. Two distinct serotypes of botulinum toxin are available for the treatment of dystonia in the US—types A and B.Botulinum Toxin Type A
Botulinum toxin type A is effective and safe, and has been shown to be more effective than medical therapy such as trihexyphenidyl in controlling symptoms of CD, with a better side-effect profile.24 Currently, three formulations of type A toxin are available in clinical practice—Botox™, Dysport, and Merz NT 201.
Botox™
The efficacy and safety of Botox has been established in several clinical trials, with 70–90% of patients with CD benefiting from this formulation.18,19,25,26 The mean dose in clinical studies was between 198 and 300 units divided among affected muscles. There is concern about the possibility of developing neutralizing antibodies with repeated therapy. In general, avoidance of high doses (above 400 units) and extending the inter-dose interval to a minimum of three months’ duration is the accepted norm. In some reports, neutralizing antibodies have been shown in up to 17% of patients, but Jankovic et al., using the current formulation of botulinum toxin type A, did not detect the presence of blocking antibodies in a threeyear, open-label observation.27 Specialized local injection techniques such as electromyogram (EMG)-guided injection may be used to increase the magnitude of benefit.28 Just prior to injection, Botox should be reconstituted using sterile non-preserved normal saline. Reconstituted medication should not be stored for more than four hours in a refrigerator as the potency is reported to wane substantially thereafter.29
The effect of Botox may be potentiated by other drugs that interfere with neuromuscular transmission, such as aminoglycoside antibiotics and other neuromuscular blockers. One study showed antagonistic action of chloroquine with botulinum toxin30 by preventing internalization of the toxin. Multiple studies have shown Botox to be a safe medication in the hands of trained physicians.18,19,25 Adverse effects such as dysphagia, neck weakness, local pain, lethargy, dysphonia, and xerostomia are temporary, but can last for weeks or months prior to waning.31
Dysport
Dysport is another A-type toxin (not available in the US) shown to be safe and effective after more than a decade of use in Europe.32,33 There are several studies comparing Botox and Dysport directly. Odergren et al. showed similar improvements and safety profiles in patients treated with Botox or Dysport.32 In 2002, Ranoux et al. demonstrated that, although Dysport had a higher incidence of adverse effects, it was more effective than Botox for both impairment and pain in CD.33 A multicenter, doubleblind, randomized controlled trial in the US recently confirmed previous reports that Dysport is safe, effective, and well-tolerated in patients with CD.34
To compare the safety, effectiveness, and duration of clinical effect of Botox and Dysport, a single-arm cross-over study was performed in 48 patients with CD, blepharospasm, and hemifacial spasm.35 This study showed that therapeutic effectiveness, safety, and duration of action are enhanced with Botox. A pivotal randomized, double-blind, placebo-controlled study of Dysport for the treatment of CD is ongoing in the US.
Merz NT 201
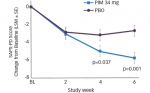
NT 201 is a new compound from Merz Pharmaceuticals. It is a lyophillized preparation of botulinum toxin type A, free of other potentially immunogenic proteins of clostridial origin. Recently, a doubleblind, non-inferiority trial compared the efficacy and safety of NT 201 with Botox in 420 patients with CD in 11 European centers.36 This study showed non-inferiority of NT 201 versus Botox with a similar safety and tolerability profile.In a separate randomized controlled trial, the efficacy and tolerability of NT 201 was compared with Botox in 14 healthy volunteers.37 After injecting four units of Botox and NT 201 into the extensor digitorum brevis muscle, reduction of compound muscle action potential was observed in both groups. The maximal effect was found between seven and 14 days, with no significant differences between groups for efficacy, time to onset of action, duration of action, and tolerability. This compound is available only in Germany, but trials are shortly planned in the US.
Botulinum Toxin Type B
Myobloc®
Myobloc® was the first toxin approved by the US Food and Drug Administration (FDA) for the treatment of CD, in December 2000. Myobloc has been shown to be effective at reducing the pain, severity, and disability associated with CD in both botulinum toxin type-A-responsive and -resistant patients.21–23,38 Botulinum toxins inhibit acetylcholine release at the neuromuscular junction by binding to receptors on pre-synaptic cholinergic nerve terminals via a multistage process.39 Myobloc specifically cleaves the synaptic vesicle-associated membrane protein (VAMP), also known as synaptobrevin.40 This cleavage blocks docking and fusion of the synaptic vesicles, a necessary step for neurotransmitter release. Botox cleaves another target protein, synaptosome-associated protein of 25kDa (SNAP 25).40 Controlled trials have shown that patients notice the benefit of Myobloc injection within four weeks, with a median duration of action between 12 and 16 weeks.41 The recommended initial dose is between 2,500 and 5,000 units, divided among injected neck muscles. Maximal reported doses have been as high as 25,000–28,000 units.42,43 Dry mouth, dysphagia, and injection site pain are the most common reported side effects with Myobloc.
Myobloc and Botox have been compared in at least two studies in both treatment-naïve patients and those previously treated with Botox. These trials revealed that both toxins provide equivalent benefit in patients with CD and have comparable side-effect profiles, except that Myobloc caused more dry mouth.44,45 Long-term prospective follow-up of patients receiving an average of 10 repeated dosing sessions of Myobloc in type-A-resistant and -responsive patients was reported.46 This study revealed that patients maintained significant efficacy over time and dry mouth diminished in frequency with repeated injection. Additional long-term use of Myobloc has been reported47 for up to 15 treatment sessions in a four-year observational study of repeated dosing with botulinum toxin type B in patients with CD. Long-term efficacy was confirmed with decreased incidence of dry mouth and dysphagia.
Summary
CD is the most common form of focal dystonia and affects more than 90,000 people in the US. Its pathophysiology is not well understood, but several hypotheses detail involvement at the central and peripheral level. In addition to sustained neck spasms, which result in an abnormal head posture, the majority of affected patients complain of head tremor and pain. One of the interesting and unique features of CD is the geste antagoniste. Several medications are used in the treatment of CD, but the efficacy of oral drug therapy is limited, with a low rate of success. Over the last decade, chemodenervation with botulinum toxin has opened a new chapter in the treatment of CD. Two types of botulinum toxin—types A and B—are being used for treatment of CD, with equivalent benefit. In cases where medical therapy fails, surgery is an option. Several trials in the US and Europe are evaluating the efficacy of deep brain stimulation (DBS) in CD. Additionally, trials evaluating the efficacy and safety of new type-A toxins are under way.