Introduction to Apomorphine and its Role in the Treatment of Parkinson’s Disease
Andrew Lees
Professor of Neurology, National Hospital for Neurology and Neurosurgery, London.
Apomorphine is a highly-potent dopamine agonist (DA) that, unlike other clinically available compounds in this class, selectively acts on both D1 and D2 dopamine receptors and has been shown in a number of published clinical trials to achieve antiparkinsonian efficacy comparable to that of orally administered levodopa.1 As far back as the 1950s, apomorphine was used to treat PD, long before its dopaminergic properties were fully understood and levodopa was developed.2 Subsequently, in the late 1960s, Cotzias and colleagues, aware of some of the shortcomings of levodopa in PD treatment, began to investigate other dopaminergic compounds and conducted clinical investigations into apomorphine in PD patients. They found that tremor responded well to apomorphine therapy, that it reduced dyskinesias in levodopa-treated patients and that it had possible anti-psychotic properties.3 The product was not developed further at that time as a therapy for PD, possibly due to both the emergence of oral dopaminergic drugs and the reluctance of neurologists to use an injectable formulation, but also due to its emetic properties. Subsequently, as a result of new pump technology in the field of diabetes and the availability of the anti-emetic domperidone, a clinical trial of apomorphine infusion for the management of Parkinsonian ON-OFF oscillations was undertaken by Stibe and colleagues.4 Published in 1988, this pivotal trial confirmed that apomorphine was the only clinically available DA that was equipotent to levodopa and it was subsequently licensed for the treatment of PD in the UK. Since that time, a range of randomised, controlled clinical trials (using apomorphine injection) and open, uncontrolled studies (using apomorphine infusion) have confirmed it as a highly effective therapy to help manage refractory motor fluctuations, with thousands of PD patients throughout the world benefitting from its use. Apomorphine infusion has also been shown to improve drug-induced dyskinesias, allowing a reduction in the oral levodopa dose.5 Nowadays, apomorphine is recognised by clinicians as an established therapy, backed by many patient-years of experience, which still has considerable value in helping to manage the complex problems they face in treating PD patients in their daily clinical practice.
This satellite symposium, held during the 18th International Congress of Parkinson’s Disease and Movement Disorders, reviewed the extensive clinical experience with subcutaneous apomorphine in PD patients that has accumulated over the past 25 years and explored why it continues to play such a valuable role in treatment of this disease.
While the management of PD focuses primarily on addressing motor symptoms, there is also a broad range of non-motor symptoms (NMS) that compromise health-related quality of life (QoL) in PD patients.6–8 In his presentation, Professor K Ray Chaudhuri discussed comparative data on both motor and non-motor effects of conventional non-oral/ transdermal therapies in advanced PD and the reported beneficial effects of subcutaneous apomorphine in this setting, particularly in terms of its side-effect profile in comparison to other agents.
Morning akinesia is a common but under-recognised symptom in PD patients, which occurs in almost 60 % of subjects9 and results from a delay in time to ON (TTO) of the first daily dose of levodopa. Professor Stuart Isaacson reviewed the interim results from the ongoing AM-IMPAKT study that demonstrate that subcutaneous apomorphine injection results in a rapid and reliable TTO in these patients, with significant improvements in QoL.
Continuous Infusion-based Drug Delivery Strategies – What is New in Comparative Data?
K Ray Chaudhuri
National Parkinson Foundation Centre of Excellence, Kings College, London
In patients with advanced PD who have severe motor complications, such as end-of-dose wearing off, unpredictable OFF or dyskinesias that can no longer be controlled by optimising oral medications, disease management becomes more challenging. These debilitating symptoms can have a significant impact on the patient’s QoL so it is important that they are treated effectively.10 Professor Chaudhuri considered that selection of the most appropriate PD therapy for an individual patient at this stage should be based on clinical evidence of therapeutic benefit.
Faced with this clinical picture, the clinician has a choice of infusional therapies, namely apomorphine continuous infusion and intrajejunal levodopa continuous infusion. Another option often considered for PD patients with advanced disease is bilateral stimulation of the subthalamic nucleus (STN-DBS). However, several other compounds are now under investigation in preclinical, or in some cases clinical, trials as options for advanced disease, including levodopa methyl ester infusion, a rotigotine once-weekly delivery system, intracerebroventricular glial cell-derived neurotrophic factor and intracerebroventricular recombinant human platelet-derived growth factor.
Professor Chaudhuri gave an overview of the range of published data confirming the benefits of apomorphine infusion in the management of advanced PD (a total of 24 studies including 552 patients) but noted that many were case series or open-label studies. Overall, study results showed a mean reduction in OFF time of 59.3 % and a mean reduction in dyskinesias of 32.5 %, which compared favourably with results reported for both intrajejunal levodopa infusion and STN-DBS. He advised that head-to-head comparisons of subcutaneous apomorphine infusion and other non-oral/transdermal therapies for advanced PD are limited but reviewed the data currently available.
Apomorphine Infusion Versus Placebo
Professor Chaudhuri noted that there are currently few data comparing apomorphine infusion and placebo. He advised that a randomised, double-blind trial, the TOLEDO study, is now underway and will include 25 centres in seven countries. Its primary objective is to investigate the efficacy of subcutaneous apomorphine infusion versus placebo in PD patients with motor fluctuations that are not well controlled by medical treatment. It is hoped that this will provide the first Level 1 evidence for the efficacy of apomorphine in this setting.
Apomorphine Infusion Versus Optimised Conventional Therapy
Data are available from an open-label, observational comparison of apomorphine infusion (n=17) with optimised conventional (oral or transdermal) therapy (n=17).11 This study was undertaken in advanced PD patients with severe dyskinesias and ON-OFF fluctuations refractory to oral therapy. After 6 months, apomorphine infusion resulted in highly significant improvements in motor scores (Unified Parkinson’s Disease Rating Scale [UPDRS] 3 [p=0.0003], UPDRS 4 [p=0.0003]), QoL measures (Parkinson’s disease questionnaire 8 [PDQ-8]; p=0.001]) and in nonmotor symptom (NMS) scores (non-motor symptoms scale [NMSS] total; p=0.0003]) (see Table 1). Notably, there were significant improvements in specific NMS such as hyperhidrosis, urinary function, fatigue, mood and sleep. In addition, apomorphine was tolerated in patients with visual hallucinations, illusions and paranoid ideations. The levodopa equivalent dose also decreased significantly in apomorphine-treated patients.
Professor Chaudhuri noted, in particular, the significant effect of apomorphine on urinary symptoms observed in this study, notably on urinary urgency, frequency and nocturia. These observations are supported by the results of preliminary studies in animal models suggesting that -8dopamine receptor agonists, particularly those which have both a D1 and D2 effect such as apomorphine, can improve bladder function.12,13 In the clinical setting, a study of 10 PD patients also confirmed that apomorphine could be a useful drug for the management of urinary symptoms. The investigators found that voiding efficiency improved after subcutaneous apomorphine injection, with an increase in mean and maximum flow rates in nine patients and a reduction in post-micturition residual volume in six.14 These preliminary findings require confirmation in larger studies.
Apomorphine Infusion versus Intrajejunal Levodopa Infusion
Treatment with apomorphine infusion plus oral levodopa has been compared with intrajejunal levodopa infusion monotherapy in a small, anecdotal study of four PD patients with motor fluctuations.15 Although not a true comparative study, the results suggested that the levodopa infusion was able to provide greater motor benefits than apomorphine infusion. More recently, as part of the Movement Disorder Society (MDS) Non-Motor Study Group, the EuroInf study, a large-scale, open-label, multicentre, international, real-life study has been undertaken to compare apomorphine infusion (n=43) with intrajejunal levodopa infusion (n=44) at 12 centres throughout the UK, Italy, Sweden, Germany, Slovenia, Austria and Denmark.16 There were no significant differences at baseline between the two groups in terms of age, gender, duration of PD, Hoehn & Yahrbased severity level, UPDRS sections III and IV, NMSS domains and total score, PDQ-8 summary index and levodopa equivalent dose.
Both treatments showed significant benefits on UPDRS part III and IV motor scores. Notably, in contrast to the previous study by Nyholm and colleagues,15 this study showed both agents to be equivalent in terms of their motor effects (see Table 2). Both compounds also had robust effects on the NMSS total score and on QoL measures (PDQ-8). When individual NMS were analysed, sleep and fatigue appeared to show greater improvements with levodopa infusion, while mood and apathy showed greater improvements with apomorphine infusion.
Professor Chaudhuri noted that when selecting therapy for PD patients it was important to take into consideration the side-effect profile of any treatment as this may affect both the overall cost of therapy and its tolerability. In the EuroInf study, after 3 years of follow-up, the most common side effect with apomorphine therapy was skin nodules. However, Professor Chaudhuri noted that none required discontinuation of therapy. He added that in his centre these were not a problem provided good skin care was exercised. Other reported adverse effects with apomorphine infusion were failure of therapy (three patients), incident impulse control disorders (ICDs; two patients) and severe somnolence (two patients), which required discontinuation of therapy in one patient. In the intrajejunal levodopa infusion arm, reported side effects included demyelinating polyneuropathy (three patients), which required discontinuation of therapy in two patients, and severe weight loss/malabsorption syndrome (seven patients), which is a late-onset effect and can occur after about 2 years of therapy. In addition, some patients experienced tube detachment and two patients developed peritonitis, one of whom subsequently died. No ICDs were observed in this treatment group and in four patients who had preexisting ICDs these were resolved. Professor Chaudhuri considered that overall apomorphine infusion therapy had the better side-effect profile of the two treatment options.
ICDs in are common in patients with PD with a reported frequency of 13.6 %,17 but few studies have been undertaken to investigate any relationship between apomorphine treatment and ICDs. Professor Chaudhuri reviewed the results of three clinical studies in PD patients treated with apomorphine where the incidence of ICDs had been reported. In a study by Garcia-Ruiz et al., of 82 PD patients treated with moderate doses apomorphine infusion, 8 % of patients reported hypersexuality after a mean follow-up period of around 20 months; this was severe in one patient who had to discontinue treatment.18 In an audit of apomorphine use in Ireland, Magennis et al. found that pre-existing ICDs were resolved in five patients after they commenced treatment.19 In a recent single-centre, observational study of 41 PD patients receiving apomorphine infusion in Professor Chaudhuri’s own institution, seven had pre-existing ICDs that resolved or attenuated after the initiation of therapy.20 Six new ICDs developed, including excessive eating, compulsive shopping and Internet use, hypersexuality and punding. However, in two cases patients were also being treated with rotigotine so the relationship between these ICDs and apomorphine is unclear. From the results, the authors concluded that apomorphine infusion appears to have a relatively low risk for the development of ICD – around 8 % which is lower than has been reported with oral DAs – with discontinuation of therapy required only in 2.4 % of cases.21
Apomorphine Infusion Versus Deep-brain Stimulation
Recognising that the mechanisms by which apomorphine continuous infusion and STN-DBS exert their therapeutic effects are very different, Alegret et al. compared the cognitive and neuropsychological outcomes of these two treatment options.22 Neuropsychological measures included Rey’s Auditory-Verbal Learning, Stroop, Trail Making, phonetic verbal fluency and Judgment of Line Orientation tests which were assessed after 6 and 12 months of treatment. In the apomorphine-treated group (n=7), no significant changes were observed in neuropsychological test performance. However, in the STN-DBS group (n=9), moderate worsening was found in phonetic verbal fluency and Stroop Naming scores. In another study, De Gaspari and colleagues compared 12-month clinical and neuropsychological outcomes following subcutaneous apomorphine infusion (n=13) or STN-DBS (n=12) in advanced PD patients.23 The investigators found that both treatments resulted in significant clinical improvement in complex PD, with STN-DBS showing greater improvements in dyskinesias. However, unlike apomorphine, STN-DBS was associated with significant worsening of neuropsychiatric inventory (NPI) scores as a result of long-term behavioural problems in some patients. The investigators subsequently reported 5-year follow-up data for this study, which confirmed the initial results.24 More recently, a study undertaken in Germany has shown that apomorphine infusion can be safely combined with DBS during surgery.25 It is recognised that perioperative withdrawal of dopaminergic medication in PD patients during DBS procedures leads to an increased risk of neurological and respiratory deterioration. In this study, data from 92 patients who underwent DBS surgery for PD were analysed retrospectively and it was found that perioperative apomorphine infusion was safe, well tolerated and resulted in a reduction in postoperative neurological deterioration and in the requirement for hospitalisation in intensive care. Based on the limited comparative data available to date, Professor Chaudhuri considered that while STN-DBS may provide better dyskinesia reduction, it is associated with worsening NPI and cognitive effects in PD patients. By contrast, apomorphine infusion is not associated with cognitive decline or NPI impairment and can also be used in the perioperative management of patients undergoing DBS surgery.
Professor Chaudhuri concluded that the results from the limited open-label comparative studies of apomorphine infusion with other therapies for complex PD suggest that it has a robust motor effect, resulting in a reduction of OFF periods comparable to that achieved with intrajejunal levodopa infusion or STN-DBS. Results from the largescale, real-life, European study, EuroInf, suggest that apomorphine infusion provides similar improvements in health-related QoL to intrajejunal levodopa infusion. However, the side-effect profile with apomorphine is superior. In addition, apomorphine infusion has been demonstrated to have beneficial non-motor effects, resulting in improvements in symptoms such sleep and urinary function while having no negative effects on hallucinations or cognition. He considered that the low rates of ICDs observed with apomorphine warrant further investigation in prospective clinical trials and that patients who have manageable ICDs can be suitable candidates for treatment with apomorphine infusion.
Delayed Time-to-ON, Morning Akinesia or Dose Failure – Oral Levodopa Response and Gastrointestinal Dysfunction
Stuart H Isaacson
Parkinson’s Disease and Movement Disorders Center of Boca Raton, Florida
Professor Isaacson continued the discussions of how apomorphine compares to levodopa, focusing in this case on the apomorphine intermittent injection. Levodopa is the gold standard of treatment for PD patients. However, while its initial effect is rapid, reliable and sustained, over time, usually around 2 to 7 years, this long-duration response is replaced by a short-duration response and as a result many patients experience OFF time. This occurs despite efforts to optimise oral therapy and the use of multiple medications. Patients experience motor fluctuations that are due not only to end-of-dose wearing off but also to delayed TTO. Until recently, the focus of treatment in this situation has been on trying to improve end-of-dose wearing off while minimising peakdose dyskinesias. However, studies now show that delayed TTO is in fact a major contributor to OFF time, being more than twice the duration of wearing off, so it is important that this aspect is also addressed to ensure that patients’ symptoms are managed quickly and reliably.26 Professor Isaacson illustrated the problem of the unreliable pharmacokinetics of levodopa and the resulting effect on the clinical response with reference to a study by Professor Fabrizio Stocchi (unpublished data) looking at levodopa plasma levels over the course of a day in a patient taking a dose every 2.5 hours. The response to each dose showed considerable variation: some doses did not increase levodopa plasma levels to within the therapeutic range, resulting in the patient being in a prolonged OFF state, whereas others produced an increase to the point where dyskinesias could occur. Delayed TTO following a levodopa dose can, therefore, result in morning akinesia, postprandial akinesia and dose failure where the dose of levodopa does not work at all.
>
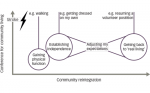
Early morning OFF (EMO) periods are common in PD patients, being reported to occur in up to 60 % of those with motor fluctuations.9,10 They are often the first manifestation of motor fluctuations and are known to have a significant negative impact on a patient’s ability to undertake daily activities and on their QoL.10 In the recent European Parkinson’s Disease Association (EUROPAR) study, the prevalence and characteristics of EMO periods were investigated in a series of 320 PD patients with a mean disease duration of seven years.9 EMO periods were found to be present in 59.7 % of patients and occurred throughout the course of the disease at all stages, in mild, moderate and severe PD patients (see Figure 1). In the patients who experienced EMO, the investigators found not only motor symptoms (morning akinesia) but also a range of NMS. A total of 88 % had EMO with mixed motor symptoms and NMS, while 12 % had pure motor EMO. The most common NMS were urinary urgency, anxiety, pain, dribbling, low mood and paresthesia, all of which complicate the clinical picture of patients with EMO.
Professor Isaacson went on to consider the reasons underlying the delayed TTO of a morning levodopa dose. It is known that the gastrointestinal (GI) system in PD patients is dysfunctional and that GI symptoms can occur even before PD is clinically diagnosed.27 Gastroparesis (delayed emptying of the stomach) is a common GI problem in patients with PD at both early and late disease stages and may be one of the underlying causes of delayed TTO.27,28 Impaired intestinal absorption may also be a contributing factor as amino acids in dietary proteins can compete with levodopa for intestinal absorption and transport across the blood–brain barrier, thus limiting its efficacy.29 However, since protein is not typically present on awakening, morning akinesia is most probably due to gastroparesis resulting in delayed gastric emptying of the dose of levodopa. Classic symptoms of gastroparesis include nausea, vomiting, early satiety, postprandial fullness and abdominal discomfort, but the presence of delayed TTO is possibly one of the major features of gastroparesis in PD, resulting from the delay in emptying of levodopa from the stomach into the proximal small intestine where it is absorbed.
In light of these GI factors in PD patients, Professor Isaacson considered that alternative formulations or routes of administration need to be considered to ensure that the PD medication is efficiently absorbed and able to exert its clinical effect. Strategies aimed at enhancing the delivery of levodopa to the proximal small intestine by the use of liquid, dispersible, modified or higher-dose levodopa have been employed. However, in PD patients who have gastroparesis, emptying of both solids and liquids may be impaired.30
Recent studies have highlighted the importance of considering pharmacokinetic factors when analysing delayed TTO. In patients with gastroparesis, the normal rise in plasma levodopa levels after oral administration has been shown to be delayed and have a lower peak, prolonging the TTO.31 The pharmacokinetics of levodopa have been investigated in 19 patients with advanced PD for more than 10 years, with and without a delayed response to the first dose in the morning.32 A significant difference was found between the maximal concentration (CMAX) values of patients with and without delayed TTO, while none of the other pharmacokinetic parameters showed any significant differences. The authors concluded that the difference in plasma concentrations between the two groups was likely to be due to delayed gastric emptying.
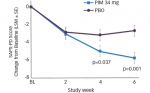
Subcutaneous apomorphine injection is one option that can be used to avoid the oral route of administration in PD patients who have gastroparesis. Apomorphine injection has previously been shown in clinical trials to provide rapid, effective relief of OFF episodes, as measured by improvements in UPDRS motor scores at 20, 40 and 90 minutes, in advanced PD patients already receiving optimised oral medication.33 The rapid onset of the effect of apomorphine injection has been clearly demonstrated in a prospective, randomised, double-blind, placebo-controlled, parallel-group study conducted at 26 US centres. The investigators found significantly greater improvements in mean UPDRS motor scores in PD patients treated with apomorphine injection versus placebo 10 minutes after administration (see Figure 2). 32
Professor Isaacson reported that the rapid and reliable therapeutic effect of apomorphine injection is being further investigated as part of the Apokyn for Motor IMProvement of Morning AKinesia Trial (AM IMPAKT) trial, an ongoing phase IV, multicentre, multiple-treatment, open-label efficacy and safety study in PD subjects with morning akinesia due to a delayed onset of levodopa effect on awakening.35 The primary objective of the study is to determine the change from baseline in average daily TTO following subcutaneous apomorphine pen injection in this patient group. Secondary endpoints include changes in the Hoehn and Yahr (H&Y) stage, clinician and patient global impression of severity and QoL as measured using the EQ-5D-3L index score and the EQ-5D-VAS visual analogue scale.
Professor Isaacson presented an interim analysis of the first 50 of a planned 100 subjects who would participate in the trial at 12 study sites in the US. Patients who had delayed TTO of a levodopa dose were identified at routine clinic visits. They recorded their TTO in a diary every 5 minutes after a morning oral levodopa dose for seven consecutive days by checking boxes either ‘yes’ or ‘no’ until onset of ON, up to 60 minutes. At the subsequent clinic visit, the optimal dose of apomorphine was then determined, defined as achieving 90 % of the levodopa response (best ON UPDRS) within 15 minutes. In 38 % of patients, the optimal dose level was 4 mg but around 18 % needed a higher dose. Patients then completed a diary for another 7 days, recording the TTO following apomorphine injection in place of the morning levodopa dose. Surprisingly, baseline demographics showed that around half of the patients were in the first decade of PD, suggesting that morning akinesia occurs early in the disease course, but also that it remains unrecognised and undertreated as the disease progresses. Many patients in the study were already taking other medications; around 60 % were taking long-acting DAs and around 40 % MAO-B inhibitors.
Following an optimal dose of apomorphine injection, baseline UPDRS OFF motor scores were found to have reduced significantly from a mean of 33.6 to 14.9 (p<0.0001). Apomorphine pen injection also significantly improved the primary endpoint of TTO and was rapid and reliable with 95 % of patients achieving at least a 20-minute reduction in TTO, with an average reduction of 40 minutes over the 7 days. Mean baseline TTO with levodopa was 60.26 minutes, which reduced significantly to 23.59 minutes with apomorphine injection. Further analysis of individual patient data demonstrates the reliability of the response to apomorphine: 48 of the 50 patients had a rapid and reliable clinical improvement in TTO. During the week when patients were taking their usual levodopa dose, dose failures were found to be surprisingly common, with 40 % having at least one during the study period. By contrast, with apomorphine injection, all but two patients achieved an ON state, 60 % of these within 20 minutes.
In terms of secondary endpoints, significant improvements were recorded in both patients’ and investigators’ ratings of global impression of severity of illness relative to akinesia/motor function before and after apomorphine therapy. Similar improvements were observed in measures of health-related QoL: EQ-5D-3L index scores were significantly reduced from a mean of 3.50 at baseline to a mean of 2.31 at the end of the 1-week apomorphine treatment period (p<0.0001) (see Figure 3). EQ- 5D-3L is a patient-reported health outcome scale related to mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension is ranked from 1 (no problem) to 5 (extreme problem) so lower scores indicate a more favourable rating. Similarly, EQ-5D VAS scores significantly improved from a mean of 48.02 at baseline to 65.25 at the end of the treatment period (p=0.0001). Using this scale, subjects rate their health state relative to akinesia on a scale of zero (worst imaginable] to 100 (best imaginable) so higher scores indicate a more favourable rating.
H&Y stage was also recorded recognising that many patients have impaired postural reflexes in the OFF state that improve when they turn ON. H&Y stage was found to be significantly reduced within 15 minutes of apomorphine compared with the baseline OFF state (2.8 versus 2.3; p<0.0001). Professor Isaacson considered that as H&Y stage was an indicator of postural instability, this change could represent an improvement in balance and a reduced risk of falling in the morning time. Overall, apomorphine pen injection was well tolerated, with the most common side effects being nausea and somnolence.
Professor Isaacson concluded that the interim results from the AM IMPAKT study confirm that subcutaneous apomorphine pen injection produces a rapid and reliable TTO in PD patients with morning akinesia due to a delayed onset of levodopa dose. Importantly, this reduction in TTO is mirrored by significant improvements in UPDRS motor score, H&Y stage, measures of QoL and global impression of severity. He cautioned, however, that this study shows that EMO periods, comprising motor symptoms such as morning akinesia and NMS, are common in PD but often go unrecognised by both patients and clinicians. The fact that OFF periods comprise not only end-of-dose wearing off but also delayed TTO reflects the problem of administering oral medication to PD patients who commonly have GI concerns. Clinicians, therefore, need to be more aware of EMO symptoms and to take steps to manage them effectively in their patients using medications that avoid the oral route of administration.