
In this narrative review, we aim to introduce the reader to the history of calcitonin gene-related peptide (CGRP) discovery and its involvement in migraine pathophysiology. We will then look at drug development and clinical trials in migraine. We will additionally discuss other headache disorders where CGRP may play a role and, last, we will discuss areas of further study.
CGRP physiology, trigeminovascular system and migraine
CGRP was first identified as a molecule in the 1980s as a nervous system RNA splicing variant produced from the calcitonin gene.1 Interestingly, even on its first discovery, the authors noted increased staining for this molecule in the nervous system, and specifically in trigeminal sensory ganglion cells.1 CGRP was found to be elevated with electrical trigeminal ganglion stimulation in humans and cats, when facial flushing was seen.2 To better characterize potential mediators of migraine attacks, a study examined the levels of vasoactive peptides in venous blood during migraine attacks, and this was the first time that CGRP was found to be elevated in the external jugular vein during a migraine attack.3,4 CGRP infusions also trigger headache, often with migrainous features, including nausea or vomiting and photophobia and phonophobia, in those with a history of migraine.5
Early evidence linking CGRP to migraine
The first migraine-targeted therapies were the triptans, which were designed to lead to vasoconstriction, targeting the vascular theory of migraine.6 These have been very successful medications and are quite effective for migraine relief.7 However, although they are vasoconstrictive medications, they have other effects. In support of the theory that CGRP is involved in migraine pain, sumatriptan lowers plasma levels of CGRP in those with pain relief, and this decrease in CGRP levels predicts the success of the therapy.3
Our understanding of the pathophysiology of migraine has evolved significantly over the last 85 years.8 The seminal work from the 1940s of Ray and Wolf first described that experimental electrical or mechanical manipulation of large intracranial arteries, dural arteries or dural venous sinuses can lead to headaches with migrainous characteristics.9 These structures are supplied by trigeminal pain sensory nerves, and as shown in Figure 1, specifically Aδ fibres with CGRP receptors, and additionally C fibres, which secrete most CGRP.10 The experimental data initially observed by Ray and Wolff may have different implications, and we have now started to regard the neurovascular complex, rather than arterial dilatation, as implicated in migraine pain generation.11,12
Figure 1: Calcitonin gene-related peptide mechanism of action
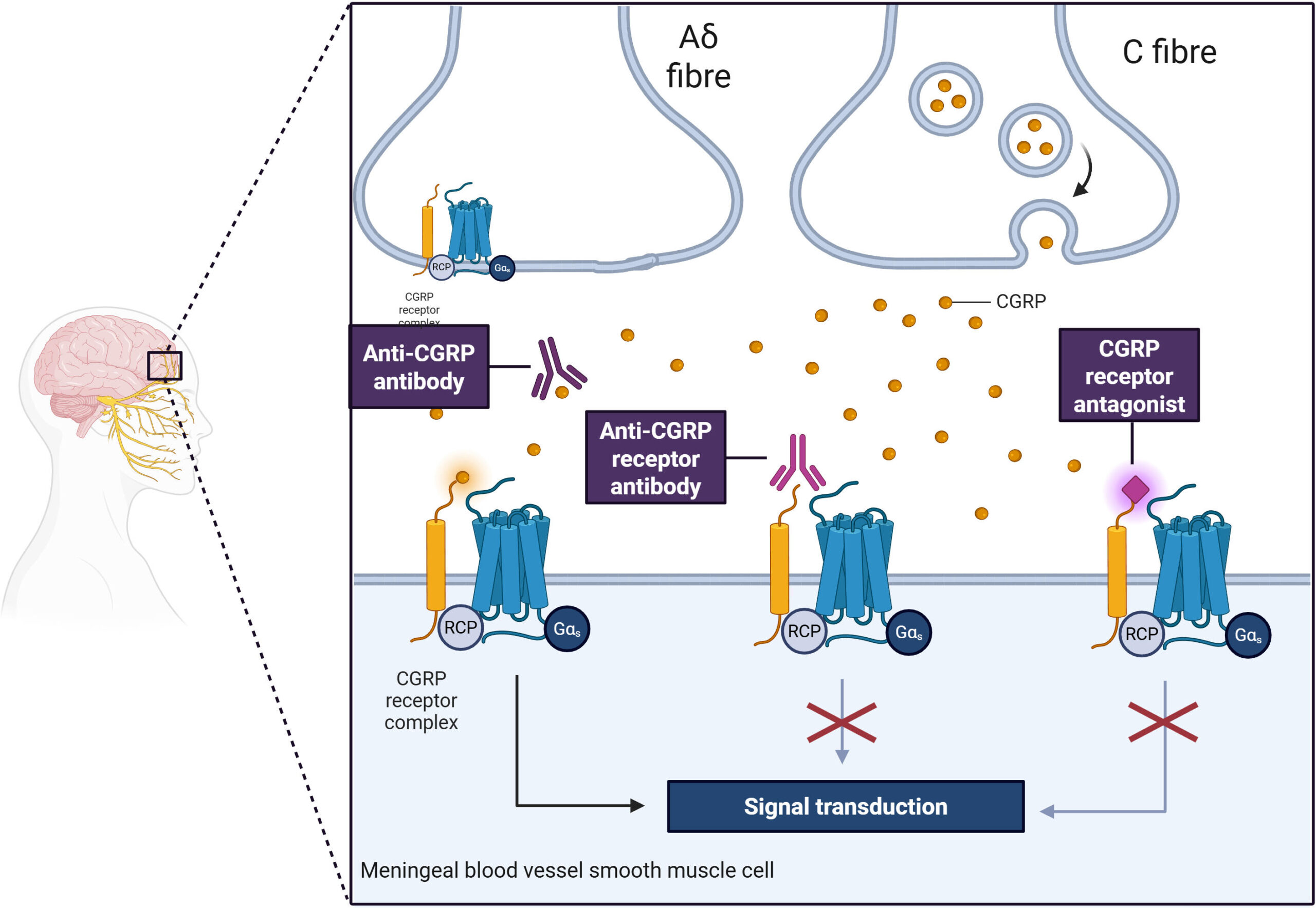
Illustration was created using https://BioRender.com
The trigeminovascular complex and the action of CGRP released from C fibres, with feedback on Aδ fibres through CGRP receptors and input on meningeal smooth muscle cells.
CGRP = calcitonin gene-related peptide; Gαs = g protein receptor subunit αs; RCP = receptor.
Development of anti–CGRP-targeted therapies
The canonical CGRP receptor (calcitonin receptor-like receptor [CLR]/receptor activity-modifying protein 1 [RAMP1] complex) and later the CGRP molecule became targets for migraine treatment.13 CGRP receptor blockade with gepants was the first target, and the first molecule described was olcegepant (BIBN4096BS; Boehringer Ingelheim Pharma KG, Ingelheim, Germany).14 In a dose–finding study, this drug was found to be effective in the acute treatment of migraine; however, this molecule was never brought to market, as an oral formulation was not possible, and its administration was intravenous.15 Telcagepant (MK-0974) was a subsequent target, and this medication also provided acute migraine relief; however, it was discontinued due to hepatotoxic effects with frequent use.16 Another target (MK-3207) was abandoned as well due to hepatotoxic effects.17 The next gepant developed, BI 33270 TA, was also proven effective in phase II data but was not developed for commercial reasons.18 The next and fifth developed drug was rimegepant (BMS-92771), which was first shown effective in a phase IIb study, and was subsequently commercialized.19 Ubrogepant and zavegepant were created next, have had pivotal studies showing efficacy and have since been commercialized.20–23 There are now three gepants, rimegepant oral, ubrogepant oral and zavegepant nasal spray, that are US Food and Drug Administration (FDA) approved for acute migraine therapy in the USA. Gepants, with the exception of zavegepant, which was only recently introduced, are widely approved as acute therapies in the European Union, UK, Canada, Australia, Japan and Singapore, with some more limited access in other countries.
The first targets against the CGRP receptor focused on acute treatment effects, given that CGRP levels were elevated during an attack. Some medications were also considered as possible migraine preventives; today, this makes sense, as we know that levels of CGRP can also be elevated interictally, especially in chronic migraine.24–26 Given these baseline CGRP level elevations between attacks, it can be postulated that they may drive the attacks, and decreasing levels may reduce the number of attacks, and these medications may work in prevention. The first study of a gepant in prevention was undertaken with rimegepant, and this was subsequently approved for episodic migraine prevention in the USA.27 Atogepant (MK-8031) is a gepant that was studied only in migraine prevention and now has indication for prevention of both episodic and chronic migraine in the USA. Atogepant is now also widely approved as preventive therapy for episodic and chronic migraine in the European Union, UK, Canada and Singapore, with some more limited access in other countries.28,29 In Table 1, we summarize indications, dosing and related side effects.30
Table 1: Anti-CGRP therapies in migraine: Dosing, indications and side effects30
| Drug dosing | Indication | Side effects |
| Acute | ||
| Ubrogepant 50–100 mg PO BID PRN | Migraine acute therapy | Nausea, drowsiness |
| Rimegepant 75 mg Q48H PO PRN | Migraine acute therapy | Nausea, drowsiness |
| Zavegepant 10 mg NS BID PRN | Migraine acute therapy | Nausea, drowsiness, dysgeusia |
| Preventive | ||
| Atogepant 10, 30 or 60 mg PO daily | Migraine prevention | Constipation, hypertension, allergic reaction |
| Erenumab 70 or 140 mg SC monthly | Migraine prevention | Injection site reactions, constipation, hypertension, Raynaud’s, alopecia, allergic reaction |
| Fremanezumab 225 mg SC monthly | Migraine prevention | Injection site reactions, constipation, hypertension, Raynaud’s, alopecia, allergic reaction |
| Galcanezumab 120 mg SC monthly, after 240 mg first month | Migraine prevention | Injection site reactions, constipation, hypertension, Raynaud’s, alopecia, allergic reaction |
| Rimegepant 75 mg Q48H PO | Episodic migraine prevention | Constipation, hypertension, allergic reaction |
BID = twice daily; CGRP = calcitonin gene-related peptide; NS = nasal spray; PO = oral; PRN = as needed; Q48H = every 48 hours; SC = subcutaneous.
The development of monoclonal antibody therapies has revolutionized medicine due to higher target specificity, decreased dosing intervals and generally few side effects.31 These CGRP-blocking monoclonal antibody medications were designed for migraine prevention, unlike the gepants, which were designed as acute therapies. The first monoclonal antibody designed to target the CGRP receptor (CLR/RAMP1 complex) was erenumab (AMG-334).32 Monoclonal antibodies against the CGRP molecule itself have also been developed: galcanezumab (LY2951742), fremanezumab (TEV-48125, formerly LBR-101) and eptinezumab (ALD403).33–35 All of these anti-CGRP receptor or ligand antibodies have shown efficacy in episodic and chronic migraine prevention and are FDA approved for the prevention of episodic and chronic migraine in the USA.36 The monoclonal antibodies against CGRP are now also widely approved as preventive therapies for episodic and chronic migraine in the European Union, UK, Canada, Australia, Japan and Singapore, with some more limited access in other countries. In Table 1, we summarize indications, dosing and related side effects.
Clinical utilization and place in therapy
These medications have been effective in both migraine acute therapy and prevention.13,36,37 Comparative studies for acute therapy of migraine show that gepants are, on average, less effective than triptans but have fewer side effects.38,39 Additionally, these medications are not known to cause cardiovascular side effects. For acute treatment of migraine, these medications are used in those who cannot tolerate triptans, or sometimes in those who have cardiovascular contraindications.40
For migraine prevention, anti-CGRP monoclonal antibodies are considered very effective and well tolerated, and there is a growing push to have these medications available as first-line therapy for individuals with migraine, so that we are no longer using older oral therapies, which are less well tolerated and possibly less effective.30,41,42 Insurance coverage for these treatments as first-line therapy is improving and, in fact, is now available in some areas based on public or private payers.
As the response to anti-CGRP therapies has been studied post-marketing, some predictors of treatment response have emerged, giving us a clue about the involved pathophysiology. Overall, patients who have a good triptan response, unilateral pain and, in some cases, unilateral autonomic symptoms tend to have better treatment response.43,44 Factors such as obesity, allodynia outside of headache attacks, everyday headache, a higher number of ineffective preventive trials (lack of treatment response) and psychiatric comorbid conditions, including depression, are predictors of those less likely to respond to treatment.43,44
Vascular concerns
Given that CGRP is a known vasodilator, there have been concerns over the cardiovascular safety of these medications from the beginning of development of this class of drugs.45 Telcagepant, which is not commercially available, was given to patients with stable coronary artery disease for acute migraine treatment and showed no increase in adverse events compared with placebo, although in a small population.45 Erenumab was similarly used in patients with known stable coronary angina, and on a treadmill test, this did not show any substantial changes in induced ischaemia between the groups, suggesting no substantial increase in cardiovascular risk in this population with erenumab use.46 Subsequently, on pivotal trials for migraine acute therapy and prevention, most studies excluded patients with cerebrovascular or cardiovascular disease.37 Looking at this entire population of patients from pivotal trials, there has been no clear increase in risk.47 Post–marketing surveillance has raised some concerns about increased risk of hypertension, possible Raynaud’s phenomenon or possible reversible cerebral vasoconstriction syndrome.48–51 The EudraVigilance database in Europe showed some possible links not reported in previous studies, including hypertension with erenumab, and atrial fibrillation and myocardial infarction with galcanezumab.52 Given these considerations, a recent article on the subject suggests that in those without substantial vascular risk factors, these medications are likely safe.53 After an acute vascular event, whether ischaemic stroke or heart attack, these medications should be stopped, and their resumptions months later may need to be considered on an individual basis, and gepants may be more prudent than longer acting therapies, such as the monoclonal antibodies, in higher risk situations.53
Studied in other headache disorders
In addition to migraine, CGRP has been studied in another headache disorder, specifically cluster headache.37,54 In cluster headache, during acute headaches, there seems to be an elevation of CGRP; however, the data on patients in the active phase of cluster headache but without headache are less conclusive, and some studies find an elevation, whereas not all studies do.54 CGRP infusion has been shown to induce cluster headache in all episodic patients during their cluster cycle, in half of chronic patients and in no patients out of cycle.55 Use of anti-CGRP therapies in cluster headache has been studied for prevention, and there was one study showing that galcanezumab at doses of 300 mg monthly (higher than for migraine) helped prevent attacks, but it was not helpful in chronic cluster headache.56,57 Notably, other anti-CGRP monoclonal antibodies had negative studies, but it remains unclear and controversial if this was due to clinical trial design rather than a lack of effect.58–61 In a case report of hemicrania continua, levels of CGRP were elevated and normalized after successful treatment with galcanezumab.62 Interestingly, CGRP release has been shown in healthy controls with capsaicin activation of V1 but not V2, suggesting that CGRP release may mediate head pain even outside of primary headache disorders.
Future directions
Future directions for the study of anti-CGRP molecules may involve better delineation of the role of CGRP in primary headache disorders, such as migraine and cluster headache. At a pathophysiological level, we understand that CGRP is secreted and utilized for signalling in the trigeminal vascular complex, but the mechanisms of headache pain generation, the chronification of headache disorders, the increased number of attacks and the role of CGRP on these parts of pathophysiology are only beginning to be understood.










